By: Trisha Kreibich, MS, Medical Illustrator/Consultant, and Robert Shepherd MS, Certified Medical Illustrator, President & CEO,
MediVisuals Inc.
This article is a continuation of a two part article on brachial plexus injury. Part 1 covered brachial plexus injuries in adults caused by a traumatic event, such as a motor vehicle collision. Part 2 will address brachial plexus injury in infants during delivery, which is also known as Shoulder Dystocia or Erb's palsy.
To review, the brachial plexus innervates the arm and is formed by several of the cervical nerve roots and the T1 nerve root. [see illustration below]
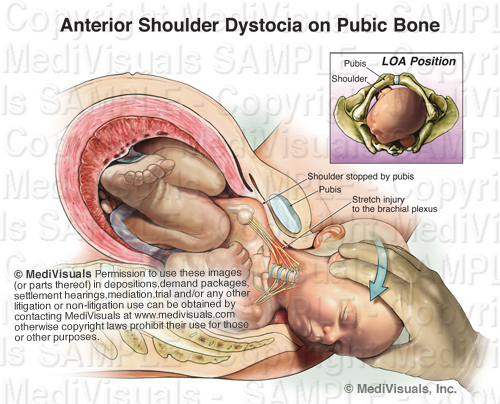
During delivery, the infant's passage through the birth canal can be stopped by the impaction of its shoulder(s) against the mother's pubic bone, sacral promontory, or both. [see illustration below]
Injury to the brachial plexus may sometimes occur because of unusually powerful uterine contractions or rapid fetal descent; however, brachial plexus injury may also result from improper obstetrician interaction. When excessive downward traction on the head of an infant with shoulder dystocia is applied (a violation of the standard of care), the delicate brachial plexus is stretched and injured. [shown below] The same may also occur when vacuum extraction is used in this situation.
As in adult brachial plexus injuries, the earlier the injury is identified and treated, the better chances are for recovery and preventing permanent damage. However, this is also dependent on the severity of the initial injury. Sometimes, an overgrowth of nerve cells (neuroma) can form around the injured nerves. When this occurs, surgical intervention and nerve grafting may be needed. [see illustration below]
There are some delivery techniques that can be used to prevent brachial plexus injury in infants with shoulder dystocia. As the illustration below demonstrates, the mother is moved to the McRoberts position, where her legs are hyperflexed to the abdomen, typically resulting in an increase of the outlet. This is often used in conjuction with an episiotomy, a cut made in the perineal body (tissue between the vagina and anus) before delivery, to enlarge the outlet and allow the obstetrician more room to perform maneuvers.
If no progress is made, moderate suprapubic pressure may be applied to free the impacted shoulder. The Wood's screw maneuver [shown below] may be used as well. This maneuver involves the obstetrician rotating the infant's anterior or posterior shoulder, and in turn the body, like a screw, freeing the impacted shoulder.
The following animation was developed to show how brachial plexus injuries can occur in a shoulder dystocia case, along with a few of the above mentioned accepted procedures that can be performed to help prevent this injury.
Reference:
Gabbe, S.G., Niebyl, J. R., & Simpson, J.L. "Obstetrics: Normal & Problem Pregnancies." 3rd ed. Philadelphia: Churchill Livingstone, 1996. 374-375, 490-494. Print.








No comments:
Post a Comment